In the challenging field of neurovascular intervention, the intricacies of pathologies are everything. In our experience, these can sometimes be some of the most difficult cases we see, including AVMs and DAVFs. Although both involve the creation of a link between an artery and a vein, the anatomy and hemodynamics, as well as the embolization of these lesions, present very different and complex problems that each require specific training. SurgeonsLab understands that this mastery of difference is key for every neurovascular fellow.
Today, we examine the details of the different characteristics of AVM and DAVF embolization and describe the key training differences between them.
Understanding the Pathologies: AVMs vs. DAVFs
Prior to describing their training differences, it's important to define both AVMs and DAVFs at a basic level.
Arteriovenous Malformations (AVMs)
AVMs are congenital lesions composed of a direct, abnormal network of blood vessels (nidus) where arteries shunt directly into veins and bypass capillaries. AVMs are mostly found in the brain parenchyma or spinal cord. High-pressure blood flowing directly into low-pressure veins leads to dilated, tortuous veins and the possibility of hemorrhage, seizure, and neurological deficit.
Dural Arteriovenous Fistulas (DAVFs)
DAVFs are acquired lesions that develop between abnormal channels linking meningeal arteries to dural venous sinuses. They are located within the dura mater, the protective layer enclosing the brain and spinal cord. Symptoms vary by site and venous drainage, including pulsatile tinnitus, visual disturbances, and intracranial hemorrhage.
Distinct Hemodynamics and Anatomical Considerations
The main distinctions in the pathologies of AVMs and DAVFs create two very different hemodynamic scenarios and anatomical problems, which directly influence the embolization strategies used for each.
AVM Embolization: Navigating the Nidus
AVM embolization generally requires access into and obliteration of the nidus itself. The object is to obliterate the abnormal shunting while preserving normal brain tissue. Catheter manipulation and introduction of embolic material must be carefully controlled, with attention to several factors.
- Microcatheterization: Entry into nidus-feeding vessels often requires navigating tiny, tortuous vessels using microcatheters. Placement of these fine wires to the target nidus is a necessary core skill.
- Embolic agent selection and delivery: Liquid agents such as nBCA or Onyx are routine. Managing the flow and penetration of these agents is crucial to achieving complete occlusion of the nidus without retrograde flow into adjacent normal arteries or loss into the draining veins.
- Flow dynamics: High flows within AVMs can cause poor catheter stability and displacement of embolic material, requiring specific flow-control techniques or staged embolization strategies.
- Risk of hemorrhage: Since AVMs are delicate and carry a significant volume of blood under pressure, rupture during the procedure is a real possibility. Fellows need the skill and training to manage this potential complication.
DAVF Embolization: Targeting the Fistula
A DAVF, on the other hand, is focused on embolizing the shunt between the dural arteries and venous sinuses to restore normal venous outflow. Access approaches and embolization strategies differ meaningfully from those used for AVMs.
- Venous vs. arterial access: Arterial access is common, but venous access (transvenous embolization) is frequently the better option for DAVFs with aggressive venous outflow. Fellows must become skilled at both approaches.
- Embolic agent deployment: Coils are often used to pack the venous side of the fistula, with liquid embolic agents filling the feeding arteries. The right approach depends heavily on the Borden or Cognard classification of the DAVF.
- Sinus preservation: Maintaining patency of normal venous sinuses, especially those participating in normal brain drainage, is critical. Fellows should master occluding the fistula without occluding the parent sinus.
- Collateral circulation: Complete occlusion can be technically difficult due to collateral arterial supply, so trainees need to identify and embolize all contributing arteries.
Realistic training for both pathologies depends on realistic simulation — as covered in more depth in our companion guide, The Comprehensive Guide to the Reusable Liquid Embolic Demonstrator.
The Role of Simulation in Mastering AVM and DAVF Embolization
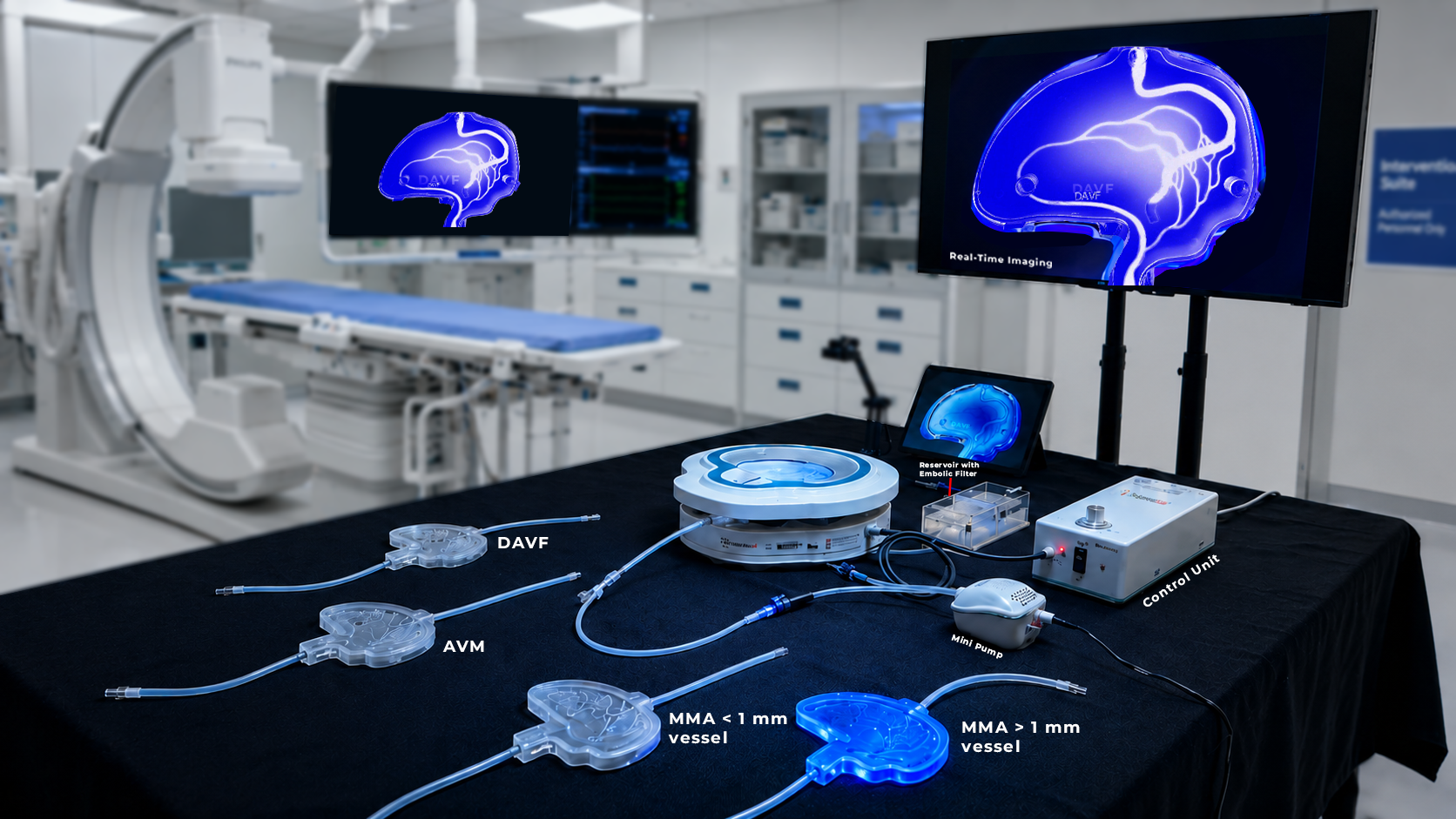
These very different problem sets cannot be solved through theoretical training alone. The procedures can only be learned through practical application in a safe, risk-free environment. For this, a sophisticated training platform like our Reusable Liquid Embolic Demonstrator is required — optimized for both AVM and DAVF embolization training.
Simulating AVM Embolization
Our AVM models simulate the intricate anatomy of the nidus with feeding and draining vessels. A fellow can practice:
- Microcatheter navigation: trailing microcatheters through tortuous feeding arteries to access the nidus.
- Embolic agent delivery: learning to achieve satisfactory nidus filling while controlling delivery flow and depth, observing behavior through the transparent model.
- Flow management: experiencing how high flow conditions affect catheter stability and delivery characteristics.
Simulating DAVF Embolization
Our DAVF models reproduce both high-flow and low-flow fistula conditions, teaching fellows:
- Dual access techniques: both transarterial and transvenous access to the fistula can be practiced.
- Coil and liquid embolic deployment: correct material selection based on DAVF classification.
- Sinus preservation strategies: occluding the fistula while maintaining normal venous outflow.
- Identifying collateral feeders: using angio-compatible features to make all feeding arteries visible to trainees.
The specialized pathology models allow fellows to acquire targeted training for specific disease states. Instant, tool-less switching between AVM and DAVF modules on a single platform permits comprehensive training across both lesion types without rebuilding the setup between sessions.
This modularity, coupled with modeled physiology, permits repeated practice of cases — building fellows' confidence and competence with both complex neurovascular diseases.
"Treating AVMs and DAVFs requires somewhat different techniques and poses separate difficulties — training has to address those differences both comprehensively and individually."
Bridging the Gap to Clinical Competence
The transition from fellow to self-sufficient neurovascular specialist requires not only academic excellence but also technical expertise, and both are demanding processes. Since treatment of AVMs and DAVFs requires different techniques and poses separate difficulties and limitations, training programs need to address these differences both comprehensively and individually.
This is exactly what the Reusable Liquid Embolic Demonstrator is designed to do: enable trainees to safely explore, practice, and learn the subtle and difficult technical maneuvers necessary to perform these life-saving procedures, building a clearer appreciation of the differences between AVM and DAVF embolization before they reach the angio suite.
Frequently Asked Questions
What are the primary differences between AVM and DAVF embolization training?
AVM embolization training consists of careful microcatheterization and accurate delivery of liquid embolic material to occlude the complex nidus located within the brain parenchyma. DAVF training consists of identifying the venous drainage and then using a combination of arterial and venous approaches, preserving the normal venous sinuses while occluding the fistulous connections.
How does the SurgeonsLab Demonstrator help differentiate AVM and DAVF embolization techniques?
The Demonstrator has specialized and interchangeable models for AVMs and DAVFs, enabling fellows to learn and practice the specific anatomical navigation, hemodynamic control, and embolic agent delivery required for each condition.
Can fellows practice both transarterial and transvenous approaches for DAVFs on the Demonstrator?
Yes. Our DAVF models support training in both transarterial and transvenous embolization techniques, allowing a thorough review of all access pathways used clinically.
What role does embolic agent selection play in AVM vs. DAVF embolization training?
Embolic material type is a key factor. The Demonstrator allows trainees to practice using liquid embolic material to close an AVM nidus, as well as coils or other agents to fill a DAVF fistula, mirroring clinical practice.
How does the Demonstrator prepare fellows for managing complications specific to AVM and DAVF embolization?
The Demonstrator offers realistic, reproducible training scenarios that include potential complications such as unintended reflux, premature occlusion, or difficult catheter navigation — giving fellows a safe environment to develop decision-making ability and confidence.